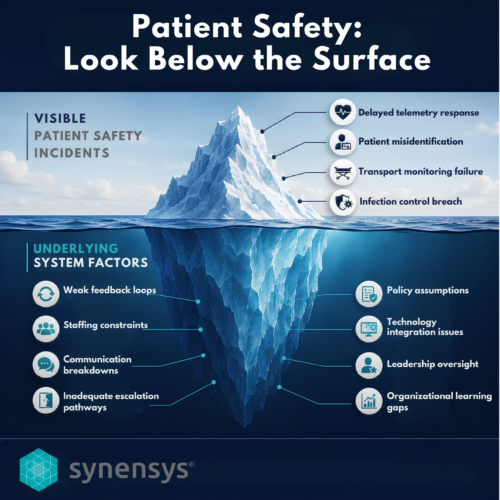
 Recent findings at a major Acute Care Hospital located in the Southeast highlight a series of patient safety incidents involving breakdowns in monitoring during transport, delayed response to telemetry alerts, patient misidentification, and infection-control gaps that exposed staff to risk. Reporting on these events also notes that regulators identified multiple contributing failures and placed the hospital in “immediate jeopardy” status due to concerns about patient harm.
Recent findings at a major Acute Care Hospital located in the Southeast highlight a series of patient safety incidents involving breakdowns in monitoring during transport, delayed response to telemetry alerts, patient misidentification, and infection-control gaps that exposed staff to risk. Reporting on these events also notes that regulators identified multiple contributing failures and placed the hospital in “immediate jeopardy” status due to concerns about patient harm.
What stands out is how easy it would be to tell this story as a list of mistakes by individuals — and how incomplete that would be.
The better question is: What system defects make these outcomes possible? The Causal Analysis based on Systems Theory (CAST) approach reminds us that the goal is not to ask who failed, but why the people involved thought they were acting safely given the information and conditions around them.
The pattern points to something deeper than isolated human error: weak feedback loops, poor coordination across handoffs, monitoring systems that inconsistently operate during transport, and a learning system that appears to react too slowly to precursor signals.
That’s why systems thinking matters in healthcare. Safety doesn’t emerge from asking people to be more careful. It emerges from designing controls, feedback loops, escalation paths, staffing models, and information systems that make the safe action the natural action. [CAST_Handb…thcare.pdf | PDF]
From a systems perspective, the deficiencies point to control and feedback problems rather than isolated frontline errors. The key safety controls appear to have depended on timely monitoring, accurate communication, adequate staffing, reliable escalation, and leadership oversight. When those controls were missing, delayed, ambiguous, or not verified, the system lost the ability to detect a deteriorating state, maintain isolation barriers, protect behavioral health patients and staff, and ensure accountability for corrective action.
If there’s one lesson here, it’s this: Traditional adverse event analyses (RCA, ACA, Gap, PRA, Fishbone, Fault Tree etc.) remain useful for reconstructing individual events and identifying event-specific contributing factors. However, the pattern of repeated immediate jeopardy findings illustrates why these methodologies alone may be insufficient when risks span multiple units, technologies, handoffs, staffing models, and governance processes. Methodologies like CAST, which implements systems thinking, would add value by identifying unsafe control actions, missing feedback loops, weak safety constraints, and flawed assumptions embedded in everyday work. Most importantly, it would shift the focus from whether individuals complied with procedures to whether the system was designed to make safe action reliable under real-world conditions (Leveson, 2019; Leveson & Thomas, 2018).
-
What failed?
When practicing CAST, we ask questions like:
-
What safety constraints were supposed to prevent this loss?
-
Where were those constraints missing, weak, or not enforced?
-
What design assumptions (policies, protocols, checklists) were incorrect or missing?